
April is off to a great start!

Gideon enjoys a reading nook at our “Happy Camper” Book Fair this month

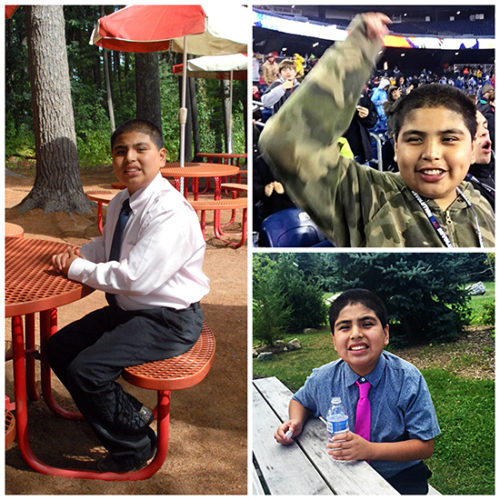
We are happy to announce Aldo as Most Improved Client of the Week!
 Aldo and his house mates completed a 6 mile walk with Aldo leading the pack. He was jogging on and off most of the way to stay ahead of the pack. Taking small breaks from time to time, but all the while wearing a smile on his face. He is becoming quite the athlete, making amazing strides in learning to roller skate and bowling strike after strike. Way to go Aldo!
Aldo and his house mates completed a 6 mile walk with Aldo leading the pack. He was jogging on and off most of the way to stay ahead of the pack. Taking small breaks from time to time, but all the while wearing a smile on his face. He is becoming quite the athlete, making amazing strides in learning to roller skate and bowling strike after strike. Way to go Aldo!
Ansel has been chosen as our Most Improved Student of the Week!
Ansel has earned this title due to his positive attitude and behavior. He has shown to be a good role model for other students, exhibiting patience and good decision-making. Ansel has earned over $400 in academic money in the last month, and has budgeted his money well. He has also been a reliable member of the boys basketball team. We are very proud of Ansel’s progress in the short time he has been at JRC. Way to go, Ansel!

Happy Birthday to Steven, Irene, Cayden, and all our students celebrating this month!

The countdown to Spring is on!

A few photos from our Valentine’s Day Dance last month!








Join us for a 6 week American Sign Language course. Session starting March 16th!
We are very happy to announce Pablo as our Academic Student of the Week.
 Pablo has been working very hard in his classroom. He has earned enough academic money to purchase a watch at the Contract Store. He has focused on a variety of tasks including computer work, reading short stories, working on counting tasks, sorting tasks, and a variety of vocational skills. Pablo has been assisting with classroom duties by passing out items to his peers throughout the day, cleaning out the refrigerator, and announcing the classroom schedule change every hour. Overall, Pablo has been doing great! Way to go!
Pablo has been working very hard in his classroom. He has earned enough academic money to purchase a watch at the Contract Store. He has focused on a variety of tasks including computer work, reading short stories, working on counting tasks, sorting tasks, and a variety of vocational skills. Pablo has been assisting with classroom duties by passing out items to his peers throughout the day, cleaning out the refrigerator, and announcing the classroom schedule change every hour. Overall, Pablo has been doing great! Way to go!